Septoplasty Knowledge Center
The complete guide to septoplasty and nasal breathing — deviated septum symptoms, septoplasty vs. rhinoplasty, nasal valve collapse, turbinate reduction, recovery, and athletic performance — from Harvard-trained plastic surgeon Dr. Mark Markarian.
Book A Virtual ConsultationWhat Is Septoplasty?
Septoplasty is a surgical procedure that straightens the nasal septum — the wall of cartilage and bone that divides the inside of the nose into two airways. When the septum is deviated (bent, crooked, or displaced to one side), it narrows one or both nasal passages and physically obstructs airflow. Septoplasty repositions and reshapes the septum back to the midline, restoring an open airway on both sides.
“A septoplasty isn't about how the nose looks — it's about how you live. When patients breathe freely for the first time in years, everything changes: sleep, energy, exercise, focus.”
— Dr. Mark Markarian, MD MSPH FACS
Unlike cosmetic rhinoplasty, septoplasty is a functional procedure — and because it treats a medical condition, it is often covered in whole or in part by health insurance. All incisions are typically made inside the nose, leaving no external scar and, in a standalone septoplasty, no change to the nose's outward appearance.
Dr. Markarian's septoplasty consultations include a detailed internal nasal examination to identify exactly where the obstruction lives — septum, turbinates, nasal valves, or all three — because a lasting result depends on treating every contributing cause, not just the most obvious one.
Septal Deviation
Time
Standalone Septoplasty
From Work
Often Covered By Insurance
Because a deviated septum is a diagnosable medical condition, septoplasty performed to correct nasal obstruction is frequently eligible for insurance coverage — verified for each patient before surgery.
Deviated Septum Symptoms
Most people with a deviated septum have lived with it so long that chronic mouth breathing, poor sleep, and one-sided congestion feel “normal.” These are the signs that your septum — not allergies alone — may be the real cause.
Common Symptoms
- Blocked nasal breathing — often worse on one side, or alternating sides when lying down
- Chronic mouth breathing — especially at night, leading to dry mouth and sore throat on waking
- Snoring and disrupted sleep — nasal obstruction is a major contributor to poor sleep quality
- Recurrent sinus infections — a deviated septum can block normal sinus drainage
- Frequent nosebleeds — airflow turbulence dries the septal lining
- Facial pressure or headaches — where the deviated septum contacts the sidewall of the nose
- Reduced exercise tolerance — being forced to mouth-breathe during exertion
A Simple Self-Check
Press one nostril closed and breathe in through the other, then switch sides. If one side is consistently and significantly harder to breathe through — day after day, congested or not — a structural cause like a deviated septum is likely and worth a proper examination.
When Sprays Stop Working
Nasal steroid sprays and antihistamines can shrink swollen tissue, but no medication can straighten bent cartilage. If you've tried medical management and still can't breathe, the obstruction is structural — and structural problems require a structural fix.
Why Patients Cannot Breathe Through Their Nose
Nasal obstruction is rarely caused by one thing. In Dr. Markarian's experience, patients who “can't breathe” usually have two or three contributing problems at once — and surgery only succeeds when every one of them is identified and addressed in the same operation.
A Deviated Septum
The dividing wall is bent or displaced, physically narrowing one or both airways. This is the most common structural cause of chronic nasal obstruction.
Enlarged Turbinates
The turbinates — humidifying structures along the nasal sidewall — enlarge in response to allergies, irritants, or to compensate for a deviated septum, further crowding the airway.
Nasal Valve Narrowing or Collapse
The nasal valves are the narrowest segments of the entire airway. Weak or narrow valve anatomy causes the sidewall to collapse inward on inspiration — exactly when you need air most.
Mucosal Swelling
Allergies, chronic inflammation, and overuse of decongestant sprays swell the nasal lining, shrinking an already narrow airway. This component is managed medically, alongside any surgical plan.
Why Diagnosis Comes First
A septoplasty that ignores collapsed nasal valves — or valve repair that ignores a deviated septum — leaves patients still unable to breathe. Dr. Markarian maps every contributing site of obstruction before planning surgery.
A Typical Patient
All Of Them
The Exam
Internal inspection of the septum and turbinates, evaluation of the nasal valves during quiet and deep inspiration, and a review of your symptom pattern — which side, which time of day, and what makes it worse.
Septoplasty vs. Rhinoplasty: What's the Difference?
The two procedures are often confused because both are “nose surgery” — but they solve entirely different problems. One changes how you breathe; the other changes how the nose looks.
Septoplasty
- Purpose: restore nasal breathing by straightening the septum
- Incisions hidden inside the nose — no external scar
- Does not change the outward shape of the nose
- Often covered by insurance as a medically necessary procedure
- Shorter recovery — most patients return to work in about a week
Rhinoplasty
- Purpose: reshape the external appearance of the nose
- Addresses humps, tip shape, width, projection, and symmetry
- Cosmetic rhinoplasty is not covered by insurance
- Swelling continues to refine for up to a year
- Explored in depth in our Rhinoplasty Knowledge Center
The Key Takeaway
If your concern is breathing, you need septoplasty (and possibly valve or turbinate work). If your concern is appearance, you need rhinoplasty. If it's both — and for many patients it is — the answer is a single combined procedure: septorhinoplasty.
Septorhinoplasty: Breathing and Aesthetics in One Surgery
Septorhinoplasty combines septoplasty and rhinoplasty into a single operation — straightening the septum and opening the airway while simultaneously refining the external shape of the nose. For patients with both a breathing problem and an aesthetic concern, combining the procedures means one surgery, one anesthesia, and one recovery instead of two.
There's also a deeper surgical logic: the septum is the central support beam of the entire nose. A crooked nose is very often the visible sign of a crooked septum, so correcting the appearance without correcting the foundation invites the deviation — and the breathing problem — to return. Dr. Markarian plans the functional and aesthetic work together so each reinforces the other.
When septorhinoplasty includes a medically necessary septoplasty, the functional portion of the procedure may be eligible for insurance coverage, reducing the overall cost of the combined surgery.
In One Operation
Instead Of Two
Why Combine Them?
The septal cartilage removed during septoplasty is also the surgeon's best grafting material for structural rhinoplasty — spreader grafts, strut grafts, and tip support — making the combined operation more efficient and more stable than staging the two separately.
Nasal Valve Collapse
The nasal valves — internal and external — are the narrowest points of the entire human airway, and they are the most frequently missed cause of persistent nasal obstruction. When the cartilage of the nasal sidewall is weak, narrow, or has been over-resected in a previous surgery, the sidewall gets sucked inward with every breath, collapsing the airway exactly when airflow demand is highest.
A classic sign: breathing improves dramatically when you pull your cheek outward, gently lift the nasal sidewall, or use adhesive breathing strips at night. If a strip fixes your breathing, your problem likely includes the valve — and a septoplasty alone will not fully solve it.
Repair involves reinforcing the weak segment with cartilage grafts — most commonly spreader grafts to widen the internal valve and alar/lateral wall grafts to stiffen the external valve — frequently performed in the same operation as septoplasty.
Internal vs. External Valve
The internal valve sits where the upper lateral cartilage meets the septum — a 10–15 degree angle that controls most nasal airflow resistance. The external valve is the nostril rim and sidewall. Either — or both — can narrow or collapse, and each requires a different repair.
The Breathing-Strip Test
If external nasal strips or gently lifting your cheek noticeably opens your breathing, mention it at consultation — it's one of the most useful clues that valve support should be part of your surgical plan.
Turbinate Reduction
The turbinates are shelf-like structures along the inner sidewall of the nose that warm, humidify, and filter the air you breathe. They are essential — but when chronically enlarged from allergies, irritants, or years of compensating for a deviated septum, the inferior turbinates can crowd the airway and cause stubborn congestion that medication no longer controls.
Turbinate reduction conservatively shrinks the enlarged turbinate — typically through a submucosal technique that reduces the tissue from the inside while preserving the functional outer lining. It is very commonly performed alongside septoplasty, since the turbinate on the “open” side of a deviated septum often enlarges over years to fill the extra space.
Conservative By Design
Turbinates should be reduced, never removed. Over-aggressive turbinate resection can permanently impair the nose's ability to humidify air. Dr. Markarian's approach preserves turbinate function while restoring the airway.
Why It's Paired With Septoplasty
Straightening the septum without reducing a compensatorily enlarged turbinate can simply shift the obstruction to the other side. Treating both in one operation is standard when both contribute.
Septoplasty Recovery Timeline
Septoplasty recovery is significantly easier than most patients expect — and easier than rhinoplasty recovery. Because the work is internal, there is typically no external bruising, no cast, and no visible sign of surgery.
Week One
Expect congestion — you'll feel stuffy, like a bad cold, as internal swelling peaks. Soft internal splints (if used) are typically removed at about one week. Most patients manage discomfort with minimal medication and return to desk work within 5–7 days.
Weeks Two to Four
Congestion steadily clears and breathing begins to open — often noticeably better than before surgery even at this stage. Light exercise usually resumes around two weeks; strenuous exercise and contact activities wait roughly 3–4 weeks with Dr. Markarian's clearance.
Months Two to Six
Internal healing completes and the full breathing benefit emerges as residual swelling of the nasal lining resolves. By this point most patients report their nasal breathing is the best it has been in years — often the best they can remember.
Recovery Guidelines
- Sleep with your head elevated for the first week to reduce swelling
- Use saline rinses as directed to keep the healing lining moist and clean
- Avoid nose blowing for the first 1–2 weeks
- Avoid strenuous exercise, heavy lifting, and bending over early on
- Attend every follow-up visit so healing is monitored closely
Dr. Markarian's Difference
Every septoplasty patient receives Dr. Markarian's private cell phone number — so recovery questions get answered the moment they come up, not at the next office visit.
Septoplasty Before & After
1 / 9 1 / 9
1 / 9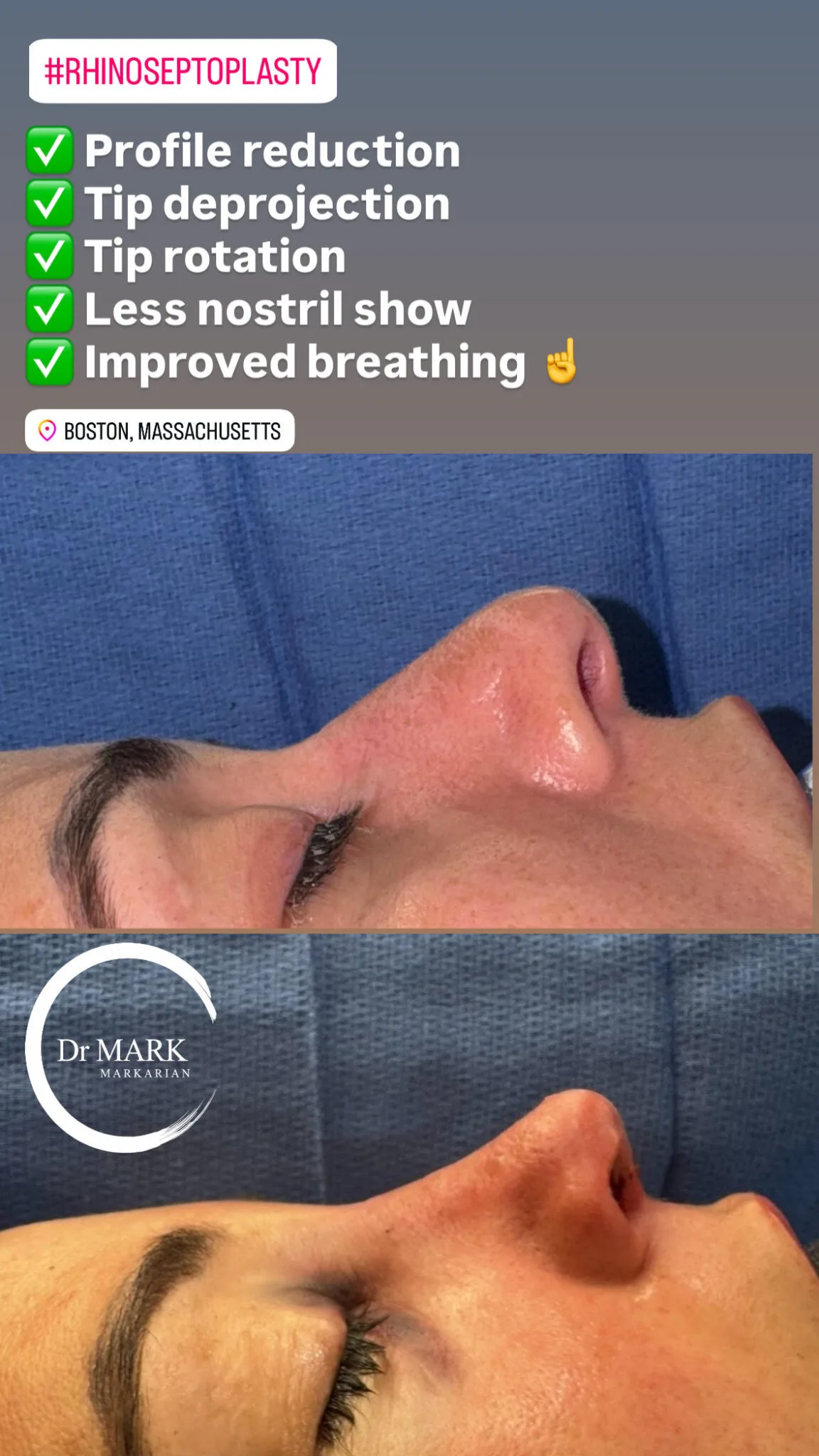 2 / 9
2 / 9 3 / 9
3 / 9 4 / 9
4 / 9 5 / 9
5 / 9 6 / 9
6 / 9 7 / 9
7 / 9 8 / 9
8 / 9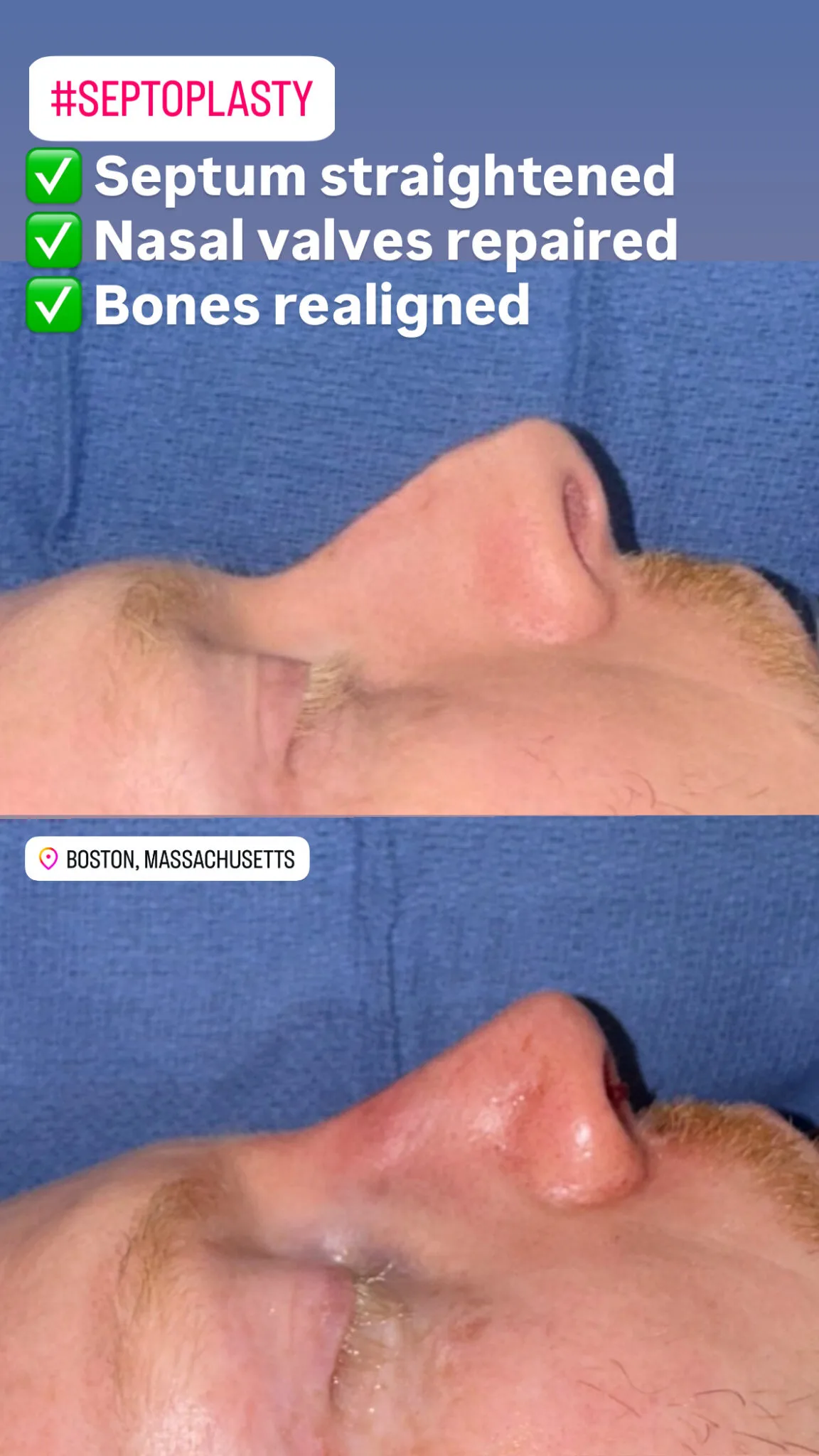 9 / 9
9 / 9Photos are of actual Dr. Markarian patients. Individual results may vary — outcomes depend on individual anatomy, the degree of septal deviation, and the specific procedures performed, and will be reviewed during your personal consultation.
“Patients are told for years that it's ‘just allergies.’ Then we straighten the septum, support the valves, and they call me a week later saying they never knew breathing could feel like this.”Dr. Mark Markarian — MD, MSPH, FACS · Harvard Aesthetic Fellowship
Functional Nasal Surgery
“Functional nasal surgery” is the umbrella term for procedures that restore how the nose works rather than how it looks: septoplasty, turbinate reduction, and nasal valve repair — performed individually or, more often, together in one operation tailored to each patient's specific sites of obstruction.
Dr. Markarian's background as a structural rhinoplasty surgeon is a genuine advantage in functional surgery. The same graft techniques that keep an aesthetic result stable for decades — spreader grafts, strut grafts, sidewall support — are exactly what keeps an airway open for decades. Function and structure are the same discipline.
One Plan, Every Cause
Septum, turbinates, and valves are examined at every functional consultation. Whatever combination is contributing to your obstruction is addressed in a single, comprehensive surgical plan — the key to a result that actually lasts.
Beyond Breathing
Patients report better sleep, less snoring, more daytime energy, improved exercise capacity, and fewer sinus infections after functional nasal surgery — benefits that compound daily for the rest of their lives.
Athletic Performance and Nasal Breathing
For athletes, nasal obstruction isn't a nuisance — it's a performance ceiling. The nose is designed to be the body's primary airway: nasal breathing filters, warms, and humidifies air, and it's where the body produces nitric oxide, a molecule that dilates blood vessels and airways and supports oxygen delivery to working muscle.
An athlete with a deviated septum or collapsing nasal valves is forced into mouth breathing at exactly the moments that matter — hard efforts, altitude, competition. Runners, cyclists, swimmers, and combat-sport athletes (whose noses have often been broken more than once) are among the patients who report the most dramatic gains after functional nasal surgery.
Restoring the nasal airway supports more efficient breathing mechanics during training, better recovery breathing between efforts, and — just as important for performance — better sleep quality every single night.
Discuss Your Breathing GoalsDuring Nasal Breathing
Full Training
A Note For Contact-Sport Athletes
Previous nasal fractures frequently cause both a deviated septum and weakened valve cartilage. Both are correctable — and timing surgery around your competitive season is part of the plan Dr. Markarian builds with you.
Septoplasty FAQs
Direct answers from Dr. Markarian to the questions patients ask most before scheduling a septoplasty consultation in Boston.
Dr. Mark Markarian
Dr. Markarian is a Harvard-trained board-certified plastic surgeon with extensive surgical experience and a rigorous academic background. His areas of particular focus include functional nasal surgery — septoplasty, nasal valve repair, and septorhinoplasty — alongside Rhinoplasty (including Ethnic Rhinoplasty), Facelifts, Necklifts, Blepharoplasty, Breast Augmentation, and Body Contouring.
What makes Dr. Markarian different? It's not just the natural results and restored breathing he delivers — it's his honesty, communication, and connection with his patients. Every patient gets his private cell phone number so they can easily reach him at any point in their surgical journey.
Breathe The Way You Were Meant To
Schedule a septoplasty consultation with Dr. Markarian to find out exactly what's blocking your breathing — and how to fix it for good.
